
So earlier this year, we talked about pain with sex (dyspareunia) and the multiple potential causes (layer by layer). Today we are going to take a deep dive (no pun intended) into one of the most pesky muscles involved in pain with sex and other symptoms of pelvic floor dysfunction.
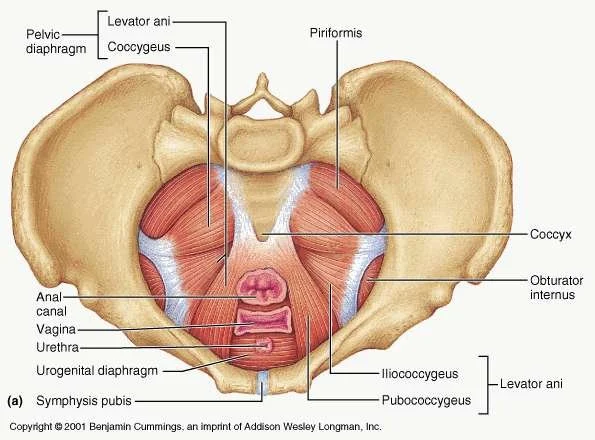
The Obturator Internus (OI) is a muscle that sits deep in the hip girdle, running from the front of the pubic bones and inserting onto the greater trochanter (the top bony part of the thigh bone).
The OI is a deep hip stabilizer, which means it helps stabilize the head of the femur (thigh bone) to keep it in socket. This muscle is also responsible for external rotation – or rolling out– of the hip and thigh. Additionally, the OI shares a fascial connection to most, if not all, of the deep pelvic floor muscles. People with dysfunction of the Obturator Internus often complete of a deep groin, hip or back pain that won’t go away with regular stretching. It is often mistaken for a Hamstring or Piriformis Dysfunction.
Just like any other muscle in the body, the Obturator Internus can become weak and too loose (hypotonic) or weak and too tight (hypertonic) over time. As we’ve talked about before, the vast majority of people with pelvic floor dysfunction fall into the second category. Sometimes this can lead to the development of trigger points (TrP) – areas of involuntarily contracted fibers in the muscle usually *very* tender to the touch. Because of this restriction, blood flow to the area is decreased, resulting in hypersensitivity to the muscle and surrounding area. The trigger points associated with OI dysfunction (OID) usually refer throughout the hip and leg.
So how is OI dysfunction evaluated and diagnosed?
As with any musculoskeletal or pelvic floor involvement, your physical therapist will take a thorough history and may ask questions to help pinpoint your symptoms. Then an objective exam will be performed that may involve assessing your back and hip mobility as strength as well as manual palpation. For OID, there are a few specifics that your therapist may look for:
Difficulty pinpointing the pain. The obturator internus has a vague referral pattern as noted above. So this may mean that sometimes you have pain over the lateral hip and then it moves to the tailbone or the sits bones.
Finding the exact location of the TrP. Your therapist may rule in OI by ruling out other muscles. They may perform deep palpation of the piriformis and hamstring to make sure that this is not your *familiar* pain – usually just medial to the sits bones.
Irritation of the pudendal nerve (which runs close to the OI) and any associated bowel or urinary frequency, urgency or overflow.
Pain with sex!
The great news is that OID can be treated by your pelvic floor PT. This may involve deep trigger point release and exercises to strengthen and stretch the Obturator Internus. This may include resisted clamshells and the frog stretch with mini cat/cows. Because the OI is so important to overall hip stability, bridges and single leg work may be included in your home program as well.
The most important thing is this: if you have back, hip or groin pain that just won’t go away — it may be good to have your obturator internus assessed. And your pelvic floor physical therapist is always around to do just that!
<3 The Recharged Performance Therapy Team
(321) 802-1630
Paige@RechargedPerformanceTherapy.com
https://www.rechargedperformancetherapy.com
References
https://www.physio-pedia.com/Obturator_Internus
https://www.youtube.com/watch?v=wYEnldl5yA0
https://my.clevelandclinic.org/health/diseases/24438-pudendal-neuralgia
Tuttle LJ, DeLozier ER, Harter KA, Johnson SA, Plotts CN, Swartz JL. The role of the obturator internus muscle in pelvic floor function. Journal of Women's Health Physical Therapy. 2016 Jan 1;40(1):15-9.
Hodges PW, McLean L, Hodder J. Insight into the function of the obturator internus muscle in humans: observations with development and validation of an electromyography recording technique. Journal of Electromyography and Kinesiology. 2014 Aug 1;24(4):489-96.